中国组织工程研究 ›› 2013, Vol. 17 ›› Issue (34): 6073-6082.doi: 10.3969/j.issn.2095-4344.2013.34.003
• 组织工程骨及软骨材料 tissue-engineered bone and cartilage materials • 上一篇 下一篇
骨水泥填充法与钢板内固定保肢治疗转移性恶性骨肿瘤
杨 俊1, 2,余 斌1,郭新辉2,杨 鹏3,张凯瑞1,张 晟1,蔡伟斌2,库建斌2,田凌彦2
- 1南方医科大学附属南方医院创伤骨科,广东省广州市 510515;2解放军第四二一医院骨科,广东省广州市 510318;3内蒙古医科大学第二附属医院,内蒙古自治区呼和浩特市 010030
-
出版日期:2013-08-20发布日期:2013-08-20 -
通讯作者:郭新辉,博士,副主任医师。解放军第四二一医院骨科,广东省广州市 510318 -
作者简介:杨俊☆,男,1977年生,辽宁省辽阳市人,南方医科大学在读博士,主治医师。
Combination of bone cement filling and plate internal fixation with limb salvage is used for metastatic malignant bone tumors
Yang Jun 1, 2, Yu Bin1, Guo Xin-hui2, Yang Peng3, Zhang Kai-rui1, Zhang Sheng1, Cai Wei-bin2, Ku Jian-bin2, Tian Ling-yan2
- 1 Department of Traumatic Orthopedics, Nanfang Hospital of Southern Medical University, Guangzhou 510515, Guangdong Province, China
2 Department of Orthopedics, the 421 Hospital of Chinese PLA, Guangzhou 510318, Guangdong Province, China
3 Second Affiliated Hospital of Inner Mongolia Medical University, Hohhot 010030, Inner Mongolia Autonomous Region, China
-
Online:2013-08-20Published:2013-08-20 -
Contact:Guo Xin-hui, M.D., Associate chief physician, Department of Orthopedics, the 421 Hospital of Chinese PLA, Guangzhou 510318, Guangdong Province, China guoxh421@163.com -
About author:Yang Jun☆, Studying for doctorate, Attending physician, Department of Traumatic Orthopedics, Nanfang Hospital of Southern Medical University, Guangzhou 510515, Guangdong Province, China; Department of Orthopedics, the 421 Hospital of Chinese PLA, Guangzhou 510318, Guangdong Province, China yangjun1267@sina.com
摘要:
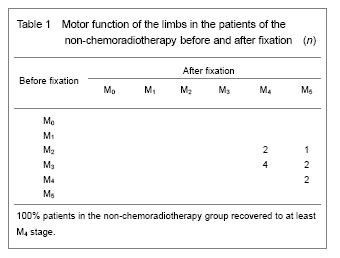
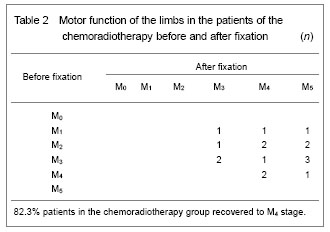
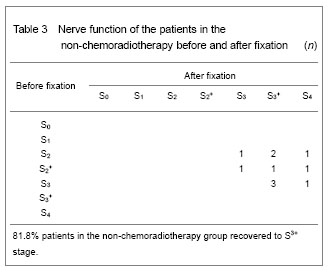
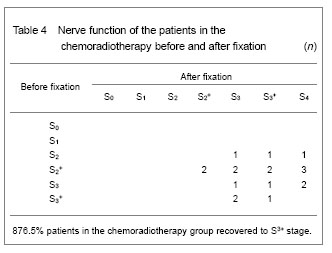
背景:目前保肢治疗已成为四肢恶性骨肿瘤的规范治疗方式,但若治疗处理不当,则会造成肿瘤复发、继发性感染、内固定或重建假体松脱等并发症。 目的:文章以传统的肢体转移性骨肿瘤外科治疗原则为基础,从四肢恶性转移性骨肿瘤患者的实际情况出发,制定人性化、个体化、简单化的姑息性治疗方案,观察骨水泥填充法结合内固定治疗转移性恶性骨肿瘤的合理性、临床疗效及预后情况。 方法:回顾分析解放军第四二一医院骨科2008年1月至2009年6月收治的恶性转移性骨肿瘤患者中筛选的31例患者,均要求保肢治疗。将31例患者按治疗方式分为2组:肿瘤清除+钢板内固定组11例,采用骨水泥填充法结合钢板内固定内固定姑息性治疗;肿瘤清除+钢板内固定+固定前放化疗组20例,采用固定前放化疗结合钢板内固定保肢治疗。全部患者固定后获4-38个月随访,平均18个月。 结果与结论:随访结果显示,肿瘤清除+钢板内固定组11例均存活、生活能自理,肢体运动功能良好;肿瘤清除+钢板内固定+固定前放化疗组20例患者中17例存活,3例分别于固定后第9,13个月因原发肿瘤的多脏器转移和自身条件较差、并发其他并发症而死亡。肿瘤清除+钢板内固定组保肢治疗后肢体神经及运动功能综合评分均较固定前提高至少1个级别以上。结果证实,对于转移性恶性骨肿瘤的保肢治疗可不采用放化疗技术,简单的骨水泥填充法结合内固定姑息性治疗的方法也有较好的效果。
中图分类号:
引用本文
杨 俊,余 斌,郭新辉,杨 鹏,张凯瑞,张 晟,蔡伟斌,库建斌,田凌彦. 骨水泥填充法与钢板内固定保肢治疗转移性恶性骨肿瘤[J]. 中国组织工程研究, 2013, 17(34): 6073-6082.
Yang Jun, Yu Bin, Guo Xin-hui, Yang Peng, Zhang Kai-rui, Zhang Sheng, Cai Wei-bin, Ku Jian-bin, Tian Ling-yan. Combination of bone cement filling and plate internal fixation with limb salvage is used for metastatic malignant bone tumors[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(34): 6073-6082.
The 28 patients were followed 9-12 months after internal fixation, with a mean period of 10.4 months. Most of the patients had significant improvement in the quality of life with the help of nutrition and symptomatic and supportive therapies: digestive ability and appetite were strengthened, limb pain and other symptoms were relieved or disappeared, the patient's psychological qualities were improved significantly, personal living skills were greatly improved, and patients felt more confident in life.
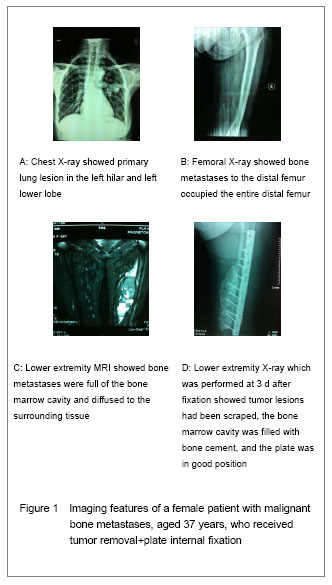
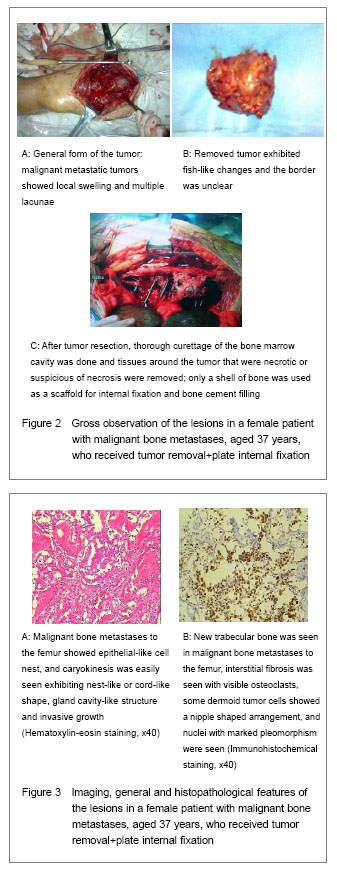
Typical cases
| [1]Xu ST, Ge BF, Xu YK. Shiyong Gukexue, 3rd. Beijing: People’s Military Publishing House. 2006.[2]Rougraff BT, Kneisel JS, Simon MA, et al. Skeletal metastases of nknown origin: a prospective study of a diagnostic strategy. Bone Joint Surg Am. 1993;75(9): 1276-1281.[3]Mankin HJ, Lange TA, Spanier SS, et al. The hazards of biopsy in patients with malignant primary bone and soft tissue tumors. J Bone Joint Surg Am. 1982;64(8): 1121- 1127.[4]Coleman RE. Skeletal complications of malignancy. Cancer. 1997;80(8 Suppl):1588-1594.[5]Wedin R, Bauer HC, Wersall P. Failures after operation for skeletal metastatic lesions of long bones. Clin Orthop Relat Res. 1999;(358):128-139.[6]Deng ZC, Chen ZG, Zahng TH, et al. Clinical analysis of the pathological fracture in femur. Zhongguo Zonghe Linchuang. 2000;16(11):828-829.[7]Salmon JM, Kilpatrick SE. Pathology of skeletal metastases. Orthop Clin North Am. 2000;31(4):537-544.[8]Sampo M, Koivikko M, Taskinen M, et al.Incidence, epidemiology and treatment results of osteosarcoma in Finland-a nationwide populationbased study. Acta Oncol. 2011;50(8):1206-1214.[9]Kabukcuoglu Y, Grimer RJ, Tillman RM, et al. Endoprosthetic replacement for primary malignant tumor of the proximal femur. Clin Orthop Relat Res. 1999;(358): 8-14.[10]Dedkov AG. Treatment outcome of patients with bone tumors after limb salvage surgery. Lik Sprava. 2010; (3-4):46-56.[11]Graci C, Maccauro G, Muratori F, et al. Infection following bone tumor resection and reconstruction with tumoral prostheses: a literature review. Int J Immunopathol Pharmacol. 2010;23(4):1005-1013.[12]Jeys LM, Grimer RJ, Carter SR, et al. Risk of amputation following limb salvage surgery with endoprosthetic replacement, in a consecutive series of 1261 patients. Int Orthop. 2003;27(3):160-163. [13]Chandrasekar CR, Grimer RJ, Carter SR, et al. Modular endoprosthetic replacement for tumours of the proximal femur. J Bone Joint Surg (Br). 2009;91(1):108-112. [14]State Council of the People’s Republic of China. Administrative Regulations on Medical Institution. 1994-09-01.[15]Wan R, Zhang WB. Treatment of metastatic bone tumor limb surgical principles. Shiyong Zhongliu Zazhi. 2008;23(4):297-300.[16]Mirels H, Metastatic disease in long bones: a proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop. 1989;(249):256-264.[17]Ye CM, Yang DS. Operation treatment of metastatic bone tumor. Shiyong Zhongliu Zazhi. 2006;21(1):12-14.[18]Ruxianai Guzhuanyi and Guxiangguan Jibing Linchuangzhenliao Zhuanjiazu. Consensus and bone metastasis of breast cancer related diseases clinical diagnosis and treatment expert. Zhonghua Zhongliu Zazhi. 2009;31(2):156-159.[19]Liu YC, Hu YC, Xia Q, et al. Management of tumorous long bone pathological fractures: Allogeneic bone reconstruction, graft reconstruction or prosthesis replacement? Zhongguo Zuzhi Gongcheng Yanjiu yu Linchuang Kangfu. 2010; (14-22):4139-4133.[20]Bacci G, Ferrari S, Mercuri M, et al. Predictive factors for local recurrence in osteosarcoma: 540 patients with extremity tumors followed for minimum 2.5 years after neoadjuvant chemotherapy. Acta Orthop Scand. 1998; 69(3):230-236.[21]Scully SP, Ghert MA, Zurakowski D, et al. Pathologic fracture in osteosarcoma: prognostic importance and treatment implications. J Bone Joint Surg (Am). 2002; 84-A(1):49-57. [22]Gupta GR, Yasko AW, Lewis VO, et al.Risk of local recurrence after deltoid-sparing resection for osteosarcoma of the proximal humerus. Cancer. 2009;115(16):3767-3773.[23]Kim HJ, Chalmers PN, Morris CD. Pediatric osteogenic sarcoma. Curr Opin Pediatr. 2010;22(1):61-66.[24]Poffyn B, Sys G, Van Maele G, et al.Radiographic analysis of extracorporeally irradiated autografts.Skeletal radiology. 2010;39(10):999-1008.[25]Zhu B. Limb salvage operation treatment of malignant bone tumor. Shiyong Gukexue. 2007;8(3):1553-1535.[26]Jing X, Wu HS, Zhou WJ. Progress in the study of pathogenesis of metastatic tumor of bone. Zhonghua Guke Zazhi. 2002;22(6):377-379.[27]Guo W, Guo Y, Feng CH. Therapeutic mechanism of bisphosphonates for metastatic tumor of bone. Zhonghua Guke Zazhi. 2003;23(1):36-38.[28]Mundy GR. Mechanisms of bone metastasis. Cancer. 1997;80(8 Suppl):1546-1556.[29]Frassica FJ, McCarthy EF. Metastatic carcinoma in bone. In pathology of bone and joint disorders. Philadelphia: WB Saunders. 1998. [30]Basset P, Bellocq JP, Wolf C, et al. A novel metalloprpteinase gene specifically expressed in stromal cells of breast carcinomas. Nature. 1990;348(6303): 699-704.[31]Yang RL, Xu WP, Guo W, et al. Surgery of metastases in limbs of 61 patients. Zhongguo Guzhongliu Gubing. 2004; (6):3330-3341.[32]Tang XD, Guo W, Yang RL, et al. Segmental allograft reconstruction in skeletal defect after limb tumor resection. Zhongguo Xiufu Chongjian Waike Zazhi. 2006;(10): 985-988.[33]Li DS, Zhang ZY, Huang MY, et al. Methods and opportunity of operation for the malignant tumor intercurrent fracture of extremity. Zhongguo Jiaoxing Waike Zazhi. 2006;(5): 331-333.[34]Gao ST, Li DS, Zhang ZY, et al. Operation modes for proximal femur tumor with pathological fracture. Zhongguo Jiaoxing Waike Zazhi. 2009;(7):488-490.[35]Sun Q, Zhao DW. Treatment of metastatic carcinoma of extremities with pathological fracture by combination of percutaneous cementaion and external fixation. Zhongguo Guzhongliu Gubing. 2005;(3):133-134.[36]Durr HR, Maier M, Pfaler M, et al. Surgical treatment of osseous metastases in patients with renal cell carcinoma. Clin Orthop. 1999;(367):283-290.[37]Raffi S, Avedian, Rex C, et al Peabody Multiplanar osteotomy with limited wide margins: a tissue preserving surgical technique for high-grade bone sarcomas. Clin Orthop Relat Res. 2010;468(10):2754-2764.[38]Fraquet N, Faizon G, Rosset P, et al. Long bones giant cells tumors: treatment by curretage and cavity filling cementation. Orthop Traumatol Surg Res. 2009;95(6): 402-406.[39]Liu J, Yang S, Li L. Department of Orthopedics Diagnosis Classification And Function Evaluation, 1st. Beijing: People’s Military Publishing House. 2012. |
| [1] | 徐 峰, 康 辉, 魏坦军, 席金涛. 椎弓根螺钉不同固定方法治疗胸腰椎骨折的生物力学分析[J]. 中国组织工程研究, 2021, 25(9): 1313-1317. |
| [2] | 张同同, 王中华, 文 杰, 宋玉鑫, 刘 林. 3D打印模型在颈椎肿瘤手术切除与重建中的应用[J]. 中国组织工程研究, 2021, 25(9): 1335-1339. |
| [3] | 陈心敏, 李文标, 熊凯凯, 熊晓燕, 郑利钦, 李木生, 郑永泽, 林梓凌. 钉道强化股骨近端防旋髓内钉治疗老年A3.3型股骨转子间骨折:最佳骨水泥量有限元分析[J]. 中国组织工程研究, 2021, 25(9): 1404-1409. |
| [4] | 杜秀鹏, 杨朝晖. 65岁以下嵌插型股骨颈骨折初始畸形程度对颈缩短的影响[J]. 中国组织工程研究, 2021, 25(9): 1410-1416. |
| [5] | 张尚普, 鞠晓东, 宋恒义, 董 智, 王 晨, 孙国栋. 关节镜下带线锚钉缝线桥缝合固定治疗肩锁关节脱位[J]. 中国组织工程研究, 2021, 25(9): 1417-1422. |
| [6] | 张 超, 吕 欣. 髋臼骨折固定后的异位骨化:危险因素、预防及其治疗进展[J]. 中国组织工程研究, 2021, 25(9): 1434-1439. |
| [7] | 周继辉, 李新志, 周 游, 黄 卫, 陈文瑶. 髌骨骨折修复内植物选择的多重问题[J]. 中国组织工程研究, 2021, 25(9): 1440-1445. |
| [8] | 陈俊名, 岳 辰, 何沛霖, 张俊涛, 孙墨渊, 刘又文. 髋关节置换与股骨近端防旋髓内钉内固定修复高龄股骨转子间骨折效果的Meta分析[J]. 中国组织工程研究, 2021, 25(9): 1452-1457. |
| [9] | 胡 凯, 乔晓红, 张永红, 王 栋, 秦泗河. 空心螺钉和钢板内固定修复移位型跟骨关节内骨折:基于15篇随机对照试验的Meta分析[J]. 中国组织工程研究, 2021, 25(9): 1465-1470. |
| [10] | 侯广原, 张继学, 张志军, 孟祥晖, 段 文, 高维陆. 骨水泥强化椎弓根螺钉内固定治疗伴骨质疏松腰椎退行性疾病的1年随访[J]. 中国组织工程研究, 2021, 25(6): 878-883. |
| [11] | 和 利, 田 维, 徐 嵩, 赵晓宇, 苗 军, 贾 健. 影响髂腰内固定治疗创伤性脊柱骨盆分离疗效的因素[J]. 中国组织工程研究, 2021, 25(6): 884-889. |
| [12] | 杨卫强, 丁 童, 杨卫可, 蒋振刚. 组合式可变应力接骨板内固定干预山羊股骨骨折断端的骨组织细胞功能及骨密度变化[J]. 中国组织工程研究, 2021, 25(6): 890-894. |
| [13] | 张 磊, 马 丽, 扶世杰, 周 鑫, 喻 林, 郭晓光. 肩关节镜下双排锚钉固定治疗肩关节前脱位伴肱骨大结节撕脱骨折[J]. 中国组织工程研究, 2021, 25(6): 895-900. |
| [14] | 袁新平, 邵艳波, 吴 超, 汪剑龄, 童梁成, 李 颖. 骨折端CT扫描参数个性化微分建模仿真目标骨段的准确性[J]. 中国组织工程研究, 2021, 25(6): 912-916. |
| [15] | 宋成杰, 常恒瑞, 石明鑫, 孟宪中. 侧方入路腰椎融合治疗后的生物力学稳定性的研究与进展[J]. 中国组织工程研究, 2021, 25(6): 923-928. |
Recent studies have shown that there is a similar survival rate between the salvage treatment and amputation in patients with metastatic malignant bone tumor, and the local recurrence rates of both the two kinds of surgical treatments are 4%-6%[8] . Currently, limb salvage therapy has become the standard treatment of malignant bone tumors manner[9] , but improper treatments can cause tumor recurrence, secondary infection, internal fixation or prosthesis loosening[10-12] , thereby resulting in the failure of limb salvage treatment. With the development of new medical treatment techniques, indications for limb salvage therapy of malignant bone tumors continue to expand, and the limb salvage rate and survival rate are both significantly increased[13] .
Design
Materials and instruments


(3) Some Chinese scholars still have disputed over the treatment of solitary bone metastases without pathological fractures as well as whether surgical treatments are recommended for different sources of metastatic bone tumors[15] . For example, generally, lung cancer patients with bone metastasis have poor prognosis, who are not advocated to receive tumor resection even if there are solitary bone metastases; while either surgical treatments or other treatments can be used to control breast cancer, prostate cancer, lymphoma, and multiple myeloma; while there is a high failure rate of local tumor resection up to 30%-40% for kidney cancer patients with bone metastases[5] , and therefore, large-segment tumor resection and reconstruction are recommended when the kidney is removed so as to obtain a better quality of life[36] . But the present study showed that in the non-chemoradiotherapy group, lung cancer, breast cancer, prostate cancer, and liver cancer patients with bone metastases were all subjected to tumor resection+internal fixation+bone cement filling; and the follow-up results showed a better outcomes of limb sensory-motor function recovery. In the chemoradiotherapy group, only chemoradiotherapy was done for limb salvage.
1 文章以传统的肢体转移性骨肿瘤外科治疗原则为基础,从四肢恶性转移性骨肿瘤患者的实际情况出发,制定人性化、个体化、简单化的姑息性治疗方案,观察骨水泥填充法结合内固定治疗转移性恶性骨肿瘤的合理性、临床疗效及预后情况。 2 结果证实,对于转移性恶性骨肿瘤的保肢治疗可以不采用放化疗技术,简单的骨水泥填充法结合内固定姑息性治疗也可为患者提供良好的生活质量和提高治疗空间。 3 文章样本量较少尚需积累,继续延长随访时间,关注固定后患者康复情况;进一步关注恶性肿瘤复发情况,积累相关信息与临床资料。
文章设计思路: 近期研究表明,保肢和截肢治疗转移性恶性骨肿瘤后患者生存率相当,而且此2种术式的局部复发率均为4%-6%。目前保肢治疗已成为四肢恶性骨肿瘤的规范治疗方式,但如若处理不当,则会造成肿瘤复发、继发性感染、内固定或重建假体松脱等并发症,导致保肢治疗失败。但随着新型医疗诊疗技术的发展,恶性骨肿瘤保肢治疗适应证不断扩展,保肢率及生存率均有显著提高。 文章以传统的肢体转移性骨肿瘤外科治疗原则为基础,从四肢恶性转移性骨肿瘤患者的实际情况出发,制定人性化、个体化、简单化的姑息性治疗方案,观察骨水泥填充法结合内固定治疗转移性恶性骨肿瘤的合理性、临床疗效及预后情况。
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||